Tuesday, May 31, 2011
NHS & Kaiser Permanente: Can we still learn?
It is amazing how planners often overlook the most important aspect of why an organisation such as Kaiser Permanente is a success. Having looked at some of their ways of saving money in my last post, I need now look at why Kaiser Permanente is such a success. New York Times
What perhaps the NHS should not ignore is one very important but simple way to contain cost: salaries for doctors, not fees.
The current thinking of containing cost in the NHS by limits set to GP Commissioning will end up in many patients not getting the essential treatments they need and GPs being blamed for poor commissioning.
Foundation Trusts will be expected to balance books or make a profit. Instead of controlling unnecessary investigation and treatment Trusts would need to treat more patients. This is not the thinking behind Kaiser Permanente and is indeed the opposite to their philosophy. It may well be fine to make money from rich overseas patients, but there is a limit as to the availability of specialist time. Ultimately NHS patients will suffer.
The side effect of the current drive of GP Commissioning is that it would no longer matter if Foundation Trusts are private or not. Before long most specialists would only offer their expert services via private organisations. Why else are the Private Health Organisations hovering around!!!
The side effect of the current drive of GP Commissioning is that it would no longer matter if Foundation Trusts are private or not. Before long most specialists would only offer their expert services via private organisations. Why else are the Private Health Organisations hovering around!!!
What can GP Commissioners do?
Do exactly what Kaiser Permanente is doing: integrate!!! Integrate primary and specialist care. Pay doctors at both levels salaries, not fees! In fact both the Mayo Clinic and the Cleveland Clinic pay their doctors salaries as well as the VA and a number of other hospitals including Johns Hopkins.
Yes, employ the specialists; buy up the hospitals and buy back pathology and other services.
Not big enough: join up with other commissioners.
What about very special services such as those provided by Royal Marsden, Queens Square, Papworth & GOS?
This can be similar to Kaiser’s arrangement with UC for kidney transplants.
But this is like the old days of Regional Health Authorities!!!
Right, did you not notice that the old black lace is back in fashion: the old black is the new black!!!
NHS-Kaiser Permanente: Summary Posts
I might as well include all the Kaiser Permanente posts:

Dec 22, 2010
Ownership and integration has undoubtedly been the hallmark of Kaiser Permanente and many observers believe that this is the main reason for its success, not so much the offering of choice to its members. Yes, members, as Kaiser Permanente is very much a Health Club, rather than an Insurer. Also, a not so well known fact is that Kaiser doctors are not allowed to practise outside the system.
It is evident that the drive to offer so called choice in the NHS, and the ensuing cross-billing, has pushed up cost
When Hospital Trusts are squeezed, true choice is no longer there. Kaiser Permanente members in fact sacrifice choice for a better value health (and life style) programme.
Jan 02, 2011
Look at major hospitals in England: Urgent Care Centres are set up and staffed by nurse practitioner, emergency nurse practitioners and GPs so that the charge by the Hospital Trusts (soon to be Foundation Trusts) for some people who tried to attend A & E could be avoided. It is often a time wasting exercise and many patients still need to be referred to the “real” A & E thus wasting much valuable time for the critically ill patients and provided fodder for the tabloid press. And payment still had to be made. Currently it is around £77.00 a go. But wait for this, over the New Year some of these Centres would employ off duty A & E Juniors to work there to save some money that Trusts could have charged.
This is certainly not how Kaiser Permanente would run things: all integrated and no such thing as “cross charging”. In fact the doctors are not on a fee-for-service basis but like Mayo Clinic, Cleveland Clinic and Johns Hopkins Hospital, doctors are paid a salary.
Feb 23, 2011
Kaiser Permanente does not cover everybody and by being able to reject or remove the chronically ill the comparison with the NHS was at best meaningless and at worst ……well I do not really want to say.
So what would they do by 2014 when they can no longer reject pre-existing conditions.
Well, their founding fathers may well have ensured their ability to continue.
Kaiser Permanent is not a Health Insurer, it is in fact a Health Maintenance Organisation. I have no doubt in my mind that they will if need be just become a Health Maintenance Club with services by amongst others, integrated primary care and secondary care doctors.
Mar 02, 2011
From one of their own advisers: Prof Chris Ham
Chris Ham"May I add something briefly? The big question is not whether GP commissioners need expert advice or patient input or other sources of information. The big problem that we have had over the past 20 years, in successive attempts to apply market principles in the NHS, has been the fundamental weakness of commissioning, whether done by managers or GPs, and whether it has been fundholding or total purchasing."
“………The barriers include government policies that risk further fragmenting care rather than supporting closer integration. Particularly important in this respect are NHS Foundation Trusts based on acute hospitals only, the system of payment by results that rewards additional hospital activity, and practice based commissioning that, in the wrong hands, could accentuate instead of reduce divisions between primary and secondary care.”
Saturday, May 28, 2011
NHS Reform: Space, Snorkel & Scotland
Sometimes in life the solution to a big problem could be so simple.
Now that David Cameron and Andrew Lansley are faced with major delays in the proposed NHS reform, the Cockroach Catcher may have a simple solution for them.
Remember the very old Urban Myth about NASA spending millions on developing a zero gravity pen:

The Myth did get into one episode of The West Wing: We Killed Yamamoto
Leo: We spent millions of dollars developing a pen for the astronauts that would work in zero gravity. Know what the Russians did?
Toby: Used a pencil?
Leo: They used a pencil.
Toby: Used a pencil?
Leo: They used a pencil.
Well it was not exactly true but it illustrated a very important point: solutions could sometimes be very simple and cheap.
Now most readers know that I love snorkeling and when I started my wife on it she, being a scientist, wanted to know the names of things she saw whilst snorkeling. The West Wing came to mind.
We used a polypropylene chopping board (the smaller one), drill a hole in the corner to tie a strap so that the hand could sometimes be free to operate the camera. We then use a golf pencil tied to the board with a fishing line to write.

Blue Brittle Star ©Am Ang Zhang 2010
So what about The NHS: A pencil solution?
Just copy Scotland; that “country” north of the border.
As much of the opposition to the new Bill is to do with the simple fact that it was a back handed way to privatise a major part of the NHS, the profitable part. Ordinary citizens without insurance will be left with a much depleted hospital service and those with insurance may find that over time they too might be dumped by their Private Health Insurers.
The Herald
JULIA HORTON
25 Feb 2009
Radical new legislation stopping private companies from running GP surgeries in Scotland is to be unveiled by ministers - further widening the divide between how the health service is run north and south of the border.
Explaining the purpose of the new legislation, which won near "unanimous" support from Scottish doctors during a recent consultation, Ms Sturgeon told The Herald: "We have decided to go ahead and legislate to effectively remove the possibility of commercial companies running GP practices.
"We want people providing GP services to be committed to the NHS and not to see it as a way of making a profit. I would hope that we would get considerable support for the bill from opposition MSPs."
The legislation, which ministers also expect to garner cross-party support, was sparked by concerns over a legal loophole which could allow into Scotland the kind of "creeping" privatisation of the NHS which is supported by the UK Government south of the border.
Trust in the government will return. There will not be any privatisation of primary or secondary care and that it would not go the way of the dental services.
Then those of us who could not afford private health care might be able to accept genuine and well thought out changes to the way the NHS will be run.
No more internal market, no more cherry picking and back to an integrated service.
By the way why not use the Scottish model that has now survived 10 years.
After devolution the NHS in England increased its reliance on a market-based approach – now one of the various controversies surrounding its future direction.
By contrast, NHS Scotland set about developing partnership agreements at national and board level as part of a strategy to engage staff in improving services.
The result, according to a study funded by the Economic and Social Research Council, is an “incredible common agenda” among interested parties from all quarters.
Research co-author Dr Peter Samuel said: “Although partnerships are found elsewhere in the public sector, NHS Scotland’s stands out as distinct and novel. It has survived for over a decade, defying reorganisation and changes in administrations, and it can offer valuable lessons in how to improve industrial relations.
By contrast, NHS Scotland set about developing partnership agreements at national and board level as part of a strategy to engage staff in improving services.
The result, according to a study funded by the Economic and Social Research Council, is an “incredible common agenda” among interested parties from all quarters.
Research co-author Dr Peter Samuel said: “Although partnerships are found elsewhere in the public sector, NHS Scotland’s stands out as distinct and novel. It has survived for over a decade, defying reorganisation and changes in administrations, and it can offer valuable lessons in how to improve industrial relations.
………Dr Samuel said: “The policymakers of NHS Scotland clearly concluded the only way to deliver better healthcare was to improve the way staff were engaged. This led to the establishment of various structures at national and local levels to give staff more say in decisions affecting their working lives and healthcare provision.
“NHS Scotland has even passed into law a ‘staff governance code’ that compels all its health boards to engage and involve staff and their representatives.
“This innovation in industrial relations is arguably one of the biggest examples of industrial democracy to be found anywhere in the world – and they have made it work.”
……….. We need to get back to using clinically relevant measures of performance that tell us how we are doing in comparison with our peers.
This has been repeatedly shown to be one of the most potent ways of modifying GP behaviour, and we should go back to it as a way of influencing clinical practice.
Scotland has no real truck with private medicine; APMS (Alternative Provider Medical Services) is not allowed. There is no market in healthcare as health boards keep primary and secondary care working together, and we actually speak to each other. Some of my best friends are consultants.
………… that trusting us to do our job is more effective than micromanagement.
Scotland: Serco NOT allowed to run GP practice
Friday, May 27, 2011
Quorum Sensing & E.Coli
As Germany
“Virulent bacteria do not want to begin secreting toxins too soon, or the host's immune system will quickly eliminate the nascent infection. Instead, Bassler explained, using quorum sensing, the bacteria count themselves and when they reach a sufficiently high number, they all launch their attack simultaneously. This way, the bacteria are more likely to overpower the immune system….” Bassler
……..many species of bacteria, including Escherichia coli MG1655, E. coli O157:H7, Salmonella typhimurium 14028, and S. typhimurium LT2 produce autoinducers similar or identical to the V. harveyi system 2 autoinducer AI-2. University of Calgary
Let us go back to an earlier post:
I am not a bacteriologist nor virologist but that did not stop me writing about these little creatures.
When I picked up the in-flight magazine on a recent flight, an article titled “Genius at Work” caught my eye. Bonnie Bassler is the bacteriologist at Princeton who discovered and pioneered the work on what she now called quorum sensing in microbes. To be more precise her initial work was with Vibrio harveyi. Vibrio is in the family of bacteria that causes Cholera. Vibrio vulnificus is carried by oysters and was most likely responsible for the serious illness of Michael Winner, film producer and now food writer of the London Sunday Times.
On following this up back home, I found an article on the website of Howard Hughes Medical Institute – she is one of the HHMI Investigators. From this article, I learned that:
“Virulent bacteria do not want to begin secreting toxins too soon, or the host's immune system will quickly eliminate the nascent infection. Instead, Bassler explained, using quorum sensing, the bacteria count themselves and when they reach a sufficiently high number, they all launch their attack simultaneously. This way, the bacteria are more likely to overpower the immune system….
For the past three hundred years……we’ve been completely wrong……we don’t know anything about bacteria until about a decade ago….”
Wow! Just as we thought we knew everything there is to know about microbes.
Bonnie Bassler will one day get the Nobel prize for medicine. You read it here first.
Fascinated, I wanted to find out more about this genius.
I would like to share with you her answers to some of questions that children were invited to ask about her life and work:
“You all asked me essentially the same question: how and when did I get interested in science. As a kid, I loved doing puzzles, solving riddles, and reading mystery books. I also loved animals and always had pets. Around high school, those interests (puzzle solving and animals) convinced me that I should be a veterinarian so I could work on mysterious illnesses in animals and cure them. In college, I realized I did not like big-bloody stuff. It became clear to me that I probably wouldn't enjoy being a vet, but I did not know what I'd do instead.
Fortunately, the vet curriculum required me to take biochemistry, genetics, and lab courses. Once I got into those classes, I fell in love with doing puzzles about little things (DNA and RNA and proteins and how they all fit together in cells). I also adored doing lab experiments and puzzling over my results. I realized that lab research was the perfect path for me. It allowed me to spend every day figuring out mysteries/puzzles that have to do with what make us alive. What could be a bigger mystery or puzzle? I changed my major in my junior year, and I have not left the lab since. (I still love animals and have a pet—Spark my cat—and I often go hiking hoping to see animals in the wild.)
I think being open-minded about what Nature is trying to tell you is the key to being creative and successful.”
Now in England
“The ability to dissect out a full set of cockroach salivary glands was a prerequisite requirement for medical school entrance in Hong Kong in our days. It is almost a 180 degree turn around nowadays when many young doctors have no idea about the biological world we live in. Nearly all Medical Schools in England

Related:
Cockroaches & Superbugs
Quorum Sensing: Cholera
NHS & Market Forces: Fund Holding & Medical Ethics
Dawn, anyone?

©Am Ang Zhang 2011
It was an interesting time during the brief few years of Fund Holding (FH). The idea that money should play no part in who gets seen was thrown out of the window. My hospital consultant colleagues all knew that preference will be given to referrals from Fund Holding practices. It was about survival. Less urgent cases would be seen if they come from FH practices.
Our Trust was small and we had to deal with two main FH practices and five non-FH ones. Child Psychiatry used to take self referrals but overnight that was stopped by our managers. Worryingly referrals from one FH practice dropped very dramatically. So the government’s clever idea may have some merit.
Then something strange happened. The other FH practice’s referrals shot up dramatically and this was across all disciplines.
Our managers thought: wow, more income for the Trust.
Not so the Cockroach Catcher and despite my protestation, I had to give their referrals preferential treatment.
“I thought it was based on clinical merit.”
Then, the bombshell: we were owed in excess of £2 million at the end of the second year and special administrator was sent in by the Authorities. We never got the extra money!
I quoted Prof. Waxman in an earlier post :
April 30, 2010 Jonathan Waxman
When I started in medicine, the hospital was run by about three people. Things were so much more simple when doctors and nurses treated patients, doing their best without the guidance of guidelines and targets, doing their best ... yes ... to make the patients better. How did we manage without forms to fill and waiting times compliance? Quite well actually. The medical director ran the medical side of things while matron and the accountant handled the rest. It wasn’t much of a business then: it didn’t have to be, because there was no internal market to manage.
The internal market’s billing system is not only costly and bureaucratic, the theory that underpins it is absurd. Why should a bill for the treatment of a patient go out to Oldham or Oxford, when it is not Oldham or Oxford that pays the bill — there is only one person that picks up the tab: the taxpayer, you and me.
And there are big problems with the billing process. For example, if a patient is seen in an outpatient clinic then there is a charge made by the hospital for his or her first attendance — but follow-up appointments are not charged. And if many treatments are given in a hospital to a patient, only the most expensive of the treatment episodes is charged.
250,000 administrative staff
There are savings to be made. It is alleged that there are just 75,000 administrators at work in the NHS but this figure is laughably mythological.
One report by the Centre for Policy Studies published in 2003 indicated that there were 250,000 administrative staff employed in the NHS: at least one administrator for every nurse.
Disempowerment
There is a general feeling in the NHS of disempowerment of the professionals. People can’t face up to the incredible struggle, the disapproval that faces any of them if they have the temerity to suggest that things should be run differently.
The principle of care for all from cradle to grave is worthy and wonderful. But the current reality is a cradle rocked by accountants who are incapable of even counting the number of times that they have rocked it. The reality is gravediggers working with a cost improvement shovel made of rust.
The Nation as a whole
Moving patients from one place to another does not save the nation’s money, though it might save a local hospital some dosh. So the internal market has failed because it does not consider the health of the nation as a whole, merely the finances of a single hospital department, a local hospital or GP practice.
So what should we do? Let us go back to the old discipline of the NHS. Let the professionals manage medicine, empower the professionals, the doctors and nurses and shove the internal market in the bin and screw down the lid. At this election time please let us hear from all political parties that they will ditch this absurd love-affair with the internal market. Instead let them help the NHS do what it does best — treat patients, and do so efficiently and economically without the crucifying expense and ridiculous parody of competition.
Why should anyone worry who provides healthcare? Because the weight of evidence is that private markets in health bring exorbitant administrative costs, lead to cherrypicking of more profitable patients, increase inequity and the postcode lottery gap, generate conflicts of interest, are unaccountable, and increase pressure for top-up payments and "care package" limits.
Keith Palmer on competition and choice
“…….competition and choice in contestable services may inadvertently cause deterioration in the quality of essential services provided by financially challenged trusts, and therefore widen the quality gap between the best and worst performers. Market forces alone will rarely drive trusts into voluntary agreement to reconfigure in ways that will improve quality and reduce costs. In most cases, the most likely outcome is that financially challenged trusts will suffer a downward spiral of continuing financial deficits, deterioration in the quality of care and a further widening of the quality gap. The NHS will have no alternative but to continue to fund these deficits or allow the trusts to fail.” RECONFIGURING HOSPITAL SERVICES: Lessons from South East London
NHS & Monitor: Toyota & McKinsey
Thursday, May 26, 2011
Wine & Tea: NHS Privatisation
As the NHS reform bill faced a delay of six months thanks to Nick Clegg, it looks like the privateers will have to wait a while longer.
Will the NHS really be privatised?
This is not the view of The Cockroach Catcher.
 As he dined with his good friend who served a beautifully fresh Red Mullet cooked the Chinese style with a simple spring onion sauce, the Cockroach Catcher produced a bottle of his recent discovery: Torrontes from Argentina.
As he dined with his good friend who served a beautifully fresh Red Mullet cooked the Chinese style with a simple spring onion sauce, the Cockroach Catcher produced a bottle of his recent discovery: Torrontes from Argentina.
Torrontes is truly an Argentinian wine that is really suitable for our Chinese Style of cooking. On the nose, it has a delicate pear and citrus flavour. My friend who is used to the good and expensive wines took a sip and declared that it has a wonderful peach flavour. It has a long aftertaste that is unusual for this class of wine. At the price, it beats any other white wine. Let us keep that as a secret.
Over tea afterwards the topic of NHS privatization came up.
No, not all of NHS will be privatized.
Why?

And some us pay taxes!!!
So nobody in their right mind would want to privatise the NHS. There is certainly more money to be made if it remained in the public domain.
Dave Cameron’s brother-in-law should not worry either as his income would go up at least 300% as long as he works for one of the private providers.
Business is business!!!
But the sums are somehow wrong!
If the private providers are making money and the GP commissioning teams have a limited pot and that Consultants working for the likes of BMI hospitals have a 300% increase in pay compared to old NHS Hospital pay scale, either tax payers are going to be forking out more and more money or someone is not going to get their treatment.
Is some politician heading for a top job with the likes of GHG or Bupa? Only time will tell and history told us it won’t be long: less than 2 years.
Will the NHS really be privatised?
This is not the view of The Cockroach Catcher.

Torrontes is truly an Argentinian wine that is really suitable for our Chinese Style of cooking. On the nose, it has a delicate pear and citrus flavour. My friend who is used to the good and expensive wines took a sip and declared that it has a wonderful peach flavour. It has a long aftertaste that is unusual for this class of wine. At the price, it beats any other white wine. Let us keep that as a secret.
Over tea afterwards the topic of NHS privatization came up.
No, not all of NHS will be privatized.
Why?
Government money is the best money for anyone to make and that is really tax payer’s money. The new NHS will be the private sector’s main source of income, as only 90,000 in the UK are covered by private insurance and often they are offered cash incentives to use the NHS.
It is therefore essential for the private health care companies that the NHS is around, at least in name, so that they can make money by providing a “better value and more competitive” service to the NHS!
Some parts of the NHS will have to remain too, as it is necessary for the private sector to dump the un-profitable patients: the chronic and the long term mentally ill, for example. (Right now, 25% of NHS psychiatric patients are treated by the private sector. But why? Even in psychiatry, there are cherries to be picked.)
Finally, in order to keep the mortality figures low at competing private hospitals, they need to be able to rush some of their patients off to NHS hospitals at the critical moments!

Have some more tea!!!
Iron Goddess of Mercy (Oolong Tea ): traditional tea of my friend's home village, Teochiu which is of course where my family is from.
These are traditional tiny cups and the tea is lovely on the nose and has a long aftertaste. To do this tea justice, use the softest water you can get: like those for a good malt!!! (Calcium is the villain here: no more than 12mg/Litre)
So the NHS will be free at the point of delivery.
Lets hope so but the money must come from somewhere.And some us pay taxes!!!
So nobody in their right mind would want to privatise the NHS. There is certainly more money to be made if it remained in the public domain.
Dave Cameron’s brother-in-law should not worry either as his income would go up at least 300% as long as he works for one of the private providers.
Business is business!!!
But the sums are somehow wrong!
If the private providers are making money and the GP commissioning teams have a limited pot and that Consultants working for the likes of BMI hospitals have a 300% increase in pay compared to old NHS Hospital pay scale, either tax payers are going to be forking out more and more money or someone is not going to get their treatment.
Is some politician heading for a top job with the likes of GHG or Bupa? Only time will tell and history told us it won’t be long: less than 2 years.
Wine Posts:
Related:
Tuesday, May 24, 2011
NHS 1978: Hope, Faith & Supermarket
It is well known that we as doctors do not have all the answers and we can only base our diagnosis and treatment on current knowledge.
Patients or their relatives are used to trust the judgement of doctors and always hope for a better or even miraculous outcome. Their faith in their doctor is often supplemented by their own religious faith.
David Cameron is no different and he has stated so on record.
I am not here to analyse his faith.
I am here to re-tell one of the stories of hope and faith I have experienced as a very junior consultant in 1978
The Mayo of the
The year was 1978 and I was employed by one of the fourteen Regional Health Authorities. The perceived wisdom was to allow consultants freedom from Area and District control that may not be of benefit to the NHS as a whole so the local Area or District Health did not hold our contracts. Even for matters like Annual Leave and Study Leave we dealt directly with RHA.
Referrals were accepted from GPs and we could refer to other specialists within the Region or to the any of the major London Centres of excellence. Many of us were trained by some of these centres and we respected them. They were the Mayos and Clevelands and Hopkins of the United Kingdom
Money or funding never came into it and we truly had a most integrated service.
We used to practice real, good and economical medicine.
We used to practice real, good and economical medicine.
The unusual cases:
Child Psychiatry like many other disciplines in medicine does not follow rules and do not function like supermarkets. Supermarkets have very advanced systems to track customer demands and they can maximise profit and keep cost down. In medicine we do sometimes get unusual cases that would have been a nightmare for the supermarket trained managers.
As it is so difficult to plan for the unusual it will become even more difficult if the present government had its way (and there is every sign that they will), not only will the reformed NHS find it difficult to cope with the unusual, it will find it extremely difficult to cope with emergencies.
Supermarket:
Why? These cases cost money and in the new world of Supermarket Styled NHS, they have to be dealt with! For that reason, not all NHS hospitals will be failed by Monitor. Some will need to be kept in order that someone could then deal with unprofitable cases. They will be the new fall guys.
But supermarkets can get things wrong too. In Spain

©Am Ang Zhang 2010
Back to the patient:
Would my patient be dealt with in the same way in 2011?
GP to Paediatrician: 13 year old with one stiff arm. Seen the same day.
Paediatrician to me: ? Psychosis or even Catatonia.
Seen same day and admitted to Paediatric Ward, DGH.
Child Psychiatrist to Gynaecologist: ? Pregnancy or tumour. Still the same day.
Gynaecologist to Radiologist: Unlikely to be pregnant, ? Ovarian cyst.
Radiologist (Hospital & no India
Gynaecologist: Operation on emergency basis with Paediatric Anaethetics Consultant. Still Day 1.
Patient unconscious and transferred to GOS on same day. Seen by various Professors.
Patient later transferred to Queen’s Square (National Hospital
Seen by more Professors.
Regained consciousness after 23 days.
Eventually transferred back to local Hospital.
None of the Doctor to Doctor decisions need to be referred to managers.
We did not have Admission Avoidance then.
How is the new Consortia going to work out the funding and how are the three Foundation Trust Hospitals going to work out the costs.
The danger is that the patient may not even get to see the first Specialist: Paediatrician not to say the second one: me.
Not to mention the operation etc. and the transfer to the Centres of excellence.
Here is an extract from my book The Cockroach Catcher: Chapter 29 The Power of Prayers
…………Something else was going on here, and I was not happy because I did not know what it was. I was supposed to know and I generally did. After all I was the consultant now.
Thank goodness she could breathe without assistance. That was the first thing I noticed. I saw mother in the corner obviously in tears. She asked if her daughter would be all right. I cannot remember what I said but knowing myself I could not have said anything too discouraging. But then I knew I was in tricky territory and it was unlikely to be the territory of a child psychiatrist.
A good doctor is one who is not afraid to ask for help but he must also know where to ask.
“Get me Great Ormond Street
“I already did.”
She is going to be a good doctor.
“Well, the Regional unit said that they had no beds so I thought I should ring up my classmate at GOS and she talked to her SR who said “send her in”.”
Who needs consultants when juniors have that kind of network? This girl will do well.
“Everything has been set up. The ambulance will be here in about half an hour and if it is all right I would like to go with her.”
“Yes, you do and thanks a lot.”
I told mother that we were transferring her daughter to the best children’s hospital inEngland
“........Ten years later mother came to see my secretary and left a photo. It was a photo of her daughter and her new baby. She had been working at the local bank since she left school, met a very nice man and now she had a baby. Mother thought I might remember them and perhaps I would be pleased with the outcome.
"I was very pleased for them too but I would hate for anyone to put faith or god to such a test too often."
David Cameron, if it was your plan not to have an integrated service, then there is not much we ordinary people could do except pray. If it was not your intention, then could you let us have an integrated service! That way you would not need many accountants and you will save money in doing so.
Just like Mayo Clinic:
“…….Mayo offers proof that when a like-minded group of doctors practice medicine to the very best of their ability—without worrying about the revenues they are bringing in for the hospital, the fees they are accumulating for themselves, or even whether the patient can pay—patients satisfaction is higher, physicians are happier, and the medical bills are lower.”
But it is probably too late:
Just like Mayo Clinic:
“…….Mayo offers proof that when a like-minded group of doctors practice medicine to the very best of their ability—without worrying about the revenues they are bringing in for the hospital, the fees they are accumulating for themselves, or even whether the patient can pay—patients satisfaction is higher, physicians are happier, and the medical bills are lower.”
But it is probably too late:
Pulse: GP consortium chairs are overwhelmingly opposed to any requirement to include hospital consultants on their boards, viewing it as a serious conflict of interest that would undermine the commissioning process, finds a Pulse survey.
King’s Fund: Million £ GP.
See also:
Monday, May 16, 2011
Photography: Point & Shoot!
Do you always need the best equipment?
Here are two taken recently in Costa Rica with a point and shoot camera:

Photomerge them in Photoshop and turn it into B & W

Now in Photoshop, use Duotone to Quadruple tone the B & W picture. Strange thing to do!
 ©Am Ang Zhang 2011
©Am Ang Zhang 2011
Here are two taken recently in Costa Rica with a point and shoot camera:

Photomerge them in Photoshop and turn it into B & W

Now in Photoshop, use Duotone to Quadruple tone the B & W picture. Strange thing to do!

Sunday, May 15, 2011
The Ruling Class: France & England

Talks on resolving the European debt crisis have been plunged into disarray after the head of the International Monetary Fund, Dominique Strauss-Kahn, was arrested and charged with sexually assaulting and attempting to rape a maid in a New York hotel.
Strauss-Kahn, 62, was taken from the first class cabin of a Paris-bound Air France flight at JFK airport by plainclothes officers before Manhattan police formally arrested him on charges of a criminal sexual act, attempted rape and unlawful imprisonment.
IMF paid for that, I suspect.
On Sunday night Anne Mansouret, a socialist regional councillor, alleged on French state TV that her daughter, the novelist Tristane Banon, had been the victim of an attempted sex attack by Strauss-Kahn in 2002 but had not gone to police. Mansouret claimed Strauss-Kahn had "a kind of addiction, a difficulty in controlling his impulses, which is a problem". She claimed his "preying" on women was a kind of "violence".
England: Thank goodness! No such news about David Cameron or Andrew Lansley.
David Laws: The Guardian
Laws was suspended from the Commons for seven days after the standards commissioner, John Lyon, ruled that over seven years he had deceived the authorities by submitting claims to pay a landlord with whom he was in a relationship and sharing a home.
The deception was serious and the sums involved substantial, Lyon said. Laws has already paid back nearly £60,000 and had to apologise to the Commons.
Lyon accepted what Laws has always claimed: that he broke the rules to protect his privacy and prevent people from finding out that he was in a gay relationship, rather than to profit, and that the way he claimed reduced the cost to the taxpayer.
We should all be grateful!!!
Chris Huhne: The Guardian
The Liberal Democrat hierarchy has defended Chris Huhne after a tape recording emerged in which the energy secretary allegedly pressed a witness not to discuss claims he had tried to avoid a driving ban.
Aides to the deputy prime minister, Nick Clegg, said they believed nothing new had surfaced to change the energy secretary's status since Vicky Pryce, from whom Huhne separated last year, made the initial claims 10 days ago. However, the local police force said it was deciding whether or not to investigate.
Looks like Wagner is worth listening to again.
Saturday, May 14, 2011
Korea & Sunshine: Golf, Music & Autism
South Korea has enjoyed its link to the west and has embraced advances in modern technology that has helped to establish itself as a major force in Steel and Car production. It is not backward in embracing modern electronic technology and is a major player in Computers, Cell Phones and of course Television.
They have a culture of taking things seriously and that shows in their attention to technical details in advance production. Why else do you think much of Apple’s iPhone4 is made by its rival, Samsung.
South Korean children were brought up to play golf and western music instruments. South Korea supplies western orchestras with a large number of musicians.
South Koreans embrace western idea of medical advance as well. Could this be the cause of one of its problems?
The Independent:
AFP
Saturday, 14 May 2011
A population-wide study of South Korean children has shown autism rates much higher than in the United States, suggesting more people worldwide may have the disorder than previously thought.
By examining 55,000 children age 7-12, even those not enrolled in special education programs, researchers found that one in 38 children had some form of autism, including the more mild social disorder known as Asperger's Syndrome.
In the United States, the autism prevalence rate is believed to be one in 110.
1: 38?
Sunshine:
In my recent cruise of Central America crossing the Panama Canal, it is not difficult to spot the South Koreans. They were dressed to be protected from the sun.
Despite temperatures reaching the mid 90s F, long sleeves, long slacks and hats with near complete surround was the order of the day; and Golf gloves as well, for both hands. And that is just for walking around town.
I have no idea how much Sunscreen they use, but that would be 50 SPF minimum.
You stay indoors with music instruments!
You stay indoors with music instruments!
So lets look at their golfers:

Very little sun tan!!!
In an earlier post:
In an earlier post:
April 1,2009
“Confirming the fears of Somali immigrants in Minneapolis, the Minnesota Health Department agreed Tuesday that young Somali children there appeared to have higher-than-usual rates of autism.
"Though health officials emphasized that their report was based on very limited data, they concluded that young Somali children appeared to be two to seven times as likely as other children to be in classes for autistic pupils.”
“Confirming the fears of Somali immigrants in Minneapolis, the Minnesota Health Department agreed Tuesday that young Somali children there appeared to have higher-than-usual rates of autism.
"Though health officials emphasized that their report was based on very limited data, they concluded that young Somali children appeared to be two to seven times as likely as other children to be in classes for autistic pupils.”
Could sunshine or the relative lack of it be the culprit here. Sunshine and Vitamin D3 is the new black.
In the history of Medicine, we sometimes ignore the most obvious. Just like mosquitoes in diseases inPanama.
Autism posts:
Friday, May 13, 2011
McKinsey: Galleon, Railtrack & The NHS
McKinsey does not make many mistakes when promoting someone to the partner level: not normally? They never make a mistake when promoting to Director level. Well, maybe not until now.
The Galleon Case
The trial of billionaire hedge fund manager Raj Rajaratnam on securities fraud charges was being watched closely both in the United States and abroad – and not just because prosecutors went after one of the top hedge fund managers in the world, but because it represented the potential for a new wave of prosecutions aimed at curtailing what many believe is a widespread practice of trading on insider information through a secret network of well-placed sources. Now that prosecutors gained convictions on all counts against Rajaratnam, expect more of these cases to come.
Mr. Kumar earned several million dollars a year as a senior executive at McKinsey. He had a gruelling work schedule, travelling some 30,000 miles a month, consulting for corporate clients across the globe.
Underpaid
In 2003, Mr. Rajaratnam, who was fast on his way to becoming a billionaire, told his business school classmate that he was underpaid.
“You work hard, travel a lot; people made fortunes while you were away and you deserve more,” he said he was told by Mr. Rajaratnam.
Mr. Kumar would later depict himself as a reluctant felon, initially rejecting Mr. Rajaratnam’s offer. But after they devised an elaborate scheme to hide the payments — opening a Swiss bank account and then transferring funds from it into a Galleon account in the name of Mr. Kumar’s housekeeper — he began moonlighting as a private consultant to Mr. Rajaratnam.
Mr. Kumar pleaded guilty to providing inside information to Mr. Rajaratnam in exchange for cash payments of at least $1.75 million from 2004 through 2009.
In the late 1990s Mr Corbett commissioned McKinsey to devise a blueprint for the company. The central recommendation that came out was that Railtrack should "sweat" its assets. This meant replacing its cyclical system of rail maintenance with a programme where infrastructure was mended on an as-and-when basis. "The theme was very much that we should get the most out of the assets before we renewed them," says a Railtrack insider.
The Independent: The might of the McKinsey mob
Network Rail: Potters Bar
Judge Bright and some of the bereaved families highlighted the fact that, as NR is a not-for-dividend company with no shareholders, any fine for NR would have to be paid from what the judge said was "an income which is substantially derived from public funds".
Perdita Kark, the daughter of Austen Kark, one of the passengers who died in the crash: said: "It's offensive that I pay a fine for something that killed my father."
Train drivers' union Aslef said it was "ludicrous that managers responsible for rail safety walked away unscathed while the public picks up a £3 million bill".
NR said it accepted the fine "as we accept the liabilities inherited from Railtrack".
NR's predecessor Railtrack was the infrastructure company in charge at the time of the crash but NR has shouldered the responsibility.
.
And now: The NHS.
David Bennett is now Chairman of Monitor and he was a Director at McKinsey & Co. In his 18 years with McKinsey he served a wide range of companies in most industry sectors, but with a particular focus on regulated, technology-intensive industries.
“It is not Greeks that could destroy the NHS, but if Monitor, the new economic regulator, is filled with competition economists with a zeal for imposing competition at every opportunity, then the NHS could be changed beyond recognition.
It is no use "liberating" the NHS from top down political control only to shackle it to an unelected economic regulator.”
Links:
Jobbing Doctor: Cracks appearing
Thank you to the Nurses, who savaged Andrew Lansley's proposals at their conference. To Colin Leys and Stewart Player for their book "the Plot against the NHS". To Allyson Pollock for all her work in exposing the marketisation of the NHS. To the bloggers (especially Jon Tomlinson at a betternhsblog, richard blogger at conservative policies dissected, Dr Grumble at Dr Grumble and there are others as well including Witch Doctor, Cockroach Catcher and Dr No) who have been pointing out the threats and absurdities. To Clare Gerada at the RCGP for a timely and vital critique.
Witch Dotor: Big Data : The next frontier
Wednesday, May 11, 2011
Monitor & Clause 56 1(a): Competition & Cartel

No clothes!!! © Am Ang Zhang 2011
Can it be so simple that David Cameron is ignorant of the pitfalls of competition in matters that concern our health or perhaps more appropriately our ill-health? Can he not see it at all or was there a different plot?
Can we really think that McKinsey could make mistakes and put the wrong person in the wrong place? They invest in people and they are everywhere.
The greatest threat to the NHS is perversely that of its regulator and in turn it is a threat to our democracy as the regulator is not elected and therefore not accountable to the electorate.
“……Tom Clark our leader writer says the real problem with the bill is the fact that the new regulator has a duty to promote competition where appropriate. He points out that in a previous life as a special adviser the regulator used his powers to squeeze state bodies in order to open up the space for private providers. It's why he is so against competition.”
For my money, the most important line in the whole of the health and social care bill is found – if I have the chapter and verse citation system right – at clause 56 1(a). It lists the first duty of the regulator Monitor, which is being transformed from the Foundation Trust hospital's overlord into being the economic regulator of the whole healthcare market, as being "promoting competition where appropriate".
The "where appropriate" sounds reassuring, but we've been here before, not least with the privatisation of the utilities, which Andrew Lansley worked on as a young civil servant, a time in his career from which he continues to draw conscious inspiration. In the beginning the 1980s utilities regulators focused on tight price regulation (RPI - X as it was called back then) to stop the former state monopolists from ripping customers off, but in time the orthodoxy changed. Particularly in electricity, market minded regulators soon made it their business to cut their charges down to size. Regulated markets, they reckoned, were never as efficient as competitive ones, so they saw it as their primary duty to restrict the market share of the old players.
Royal Mail & PostComm
When Labour set the Royal Mail on a new commercial footing, around a decade ago, it set up a regulator, PostComm, which was also charged with promoting competition to the extent it was desirable, and as a special adviser at the Department for Trade and Industry in 2005-06 I saw the miserable consequences up close. Instead of straightforwardly capping stamp prices, as one might expect, the regulator warned Royal Mail not to cut prices in those markets too aggressively in those markets (notably bulk market mail) where it faced stiff competition from new commercial entrants. The aim was to lever these new players into the market until they achieved a truly significant slice of the pie, and the Mail's hands were tied to ensure that this happened. Only then, the regulator reasoned, would competition become real, and so only then would the magic of the market work.
Well, perhaps there have been benefits for bulk mail customers, I am in no position to judge, but I don't think many would claim that there have been many benefits for the Royal Mail itself. It has limped from one crisis to the next, and then on to bailout and now finally towards privatisation.
Pro-competition mania at Monitor
There have been troubling noises, including at one point from Vince Cable, about how the universal one-price tariff can be protected. But these problems are of nothing compared to what would happen to our hospitals if the pro-competition mania got entrenched at Monitor.
Unelected Regulators
The unelected regulators, who regard themselves as beyond the reach of elected politicians, might turn out to be sensible people. But if they turned out to be the type to dance with dogma, then they could end up making it their mission to give new private players some particular percentage of the new healthcare market, which would of course mean denying the same volume of work to NHS hospitals. And that would have the unavoidable corollary of forcing a good number of them to the wall. NHS training arrangements, the integration of care and a decent geographical spread of provision could all go to the wall with them in tandem. No doubt there are safeguards, but wouldn't it be better to recast the bill, so that the regulators were charged merely with "overseeing" competition where it exists, as opposed to actively promoting it? After all, as any medic can tell you, prevention is better than cure.
Competition & Cartels
Let us see what competition led to in the Airline industry: Cartels, cartels and more cartels!!!
According to federal prosecutors, when the airline industry took a nose dive a decade ago industry executives tried to fix it, with a massive price-fixing scheme among airlines the world over, that artificially inflated passenger and cargo fuel surcharges to help companies make up for lost profits. Convicted airlines include British Airways, Korean Air, and Air France-KLM.
The Lufthansa and Virgin Atlantic mea culpas allowed them to take advantage of a Justice Department leniency program because they helped crack the conspiracies.
The European Commission has fined 11 airlines almost 800m euros (£690m) for fixing the price of air cargo between 1999 and 2006.
British Airways was fined 104m euros, Air France-KLM 340m euros and Cargolux Airlines 79.9m euros.
The fines follow lengthy investigations by regulators in Europe, the US and Asia, dating back to 2006.
The EU said that the airlines "co-ordinated their action on surcharges for fuel and security without discounts", between early 1999 and 2006.
Singapore Airlines 74.8m
SAS 70.2m
Cathay Pacific 57.1m
These are some of the most respected names in the industry!!!
NHS & The Mayo Model: What if!
“The best interest of the patient is the only interest to be considered.”
Tuesday, May 10, 2011
Photography: Best lens for portrait & landscape!

It is not so difficult to say what the best portrait lens is. You want a medium telephoto lens from 85 mm through 105mm and 135mm. You pick the widest aperture you can afford and that may mean 85/1.2 at great expense. The background could be so well blurred that you do not need a studio back drop. My favourite is of course the 180/2.8.
with 180/2.8 Taken in France.
© Am Ang Zhang 2005
Now, when it comes to landscape, I am going to go against the grain (in true Cockroach Catcher style) and suggest something different.
So you are not recommending the 18 mm superwide then.
No!!!
250mm.
What? That is a telephoto lens! I thought that should be for birds and safari.
May well be.
But because of the better resolution, you have situations where you can make use of it.
But such a narrow angle of view?
Ah! But you can take a number of photos and stitch them together. You can use either Photoshop or there are free softwares including one from Microsoft that can be used for panoramic merging.
Here are 4 photos I took on my recent cruise. We reached Panama at dawn.

Four straight shots with 250mm lens © Am Ang Zhang 2011

Oooops here is a nice boat © Am Ang Zhang 2011

Put them through Photoshop© Am Ang Zhang 2011

Move the boat up© Am Ang Zhang 2011
Some minor photoshopping

Panama © Am Ang Zhang 2011
Photography:
Monday, May 9, 2011
David Cameron: More listening
Again from one of yours:
Keith Palmer
All four DGHs in South East London were in chronic financial deficit, despite rapid growth in both NHS funding and hospital activity. In 2005/6 the aggregate underlying deficit of the four DGHs was more than £50 million and legacy debt exceeded £160 million. Analysis undertaken at the time indicated that they were expected to remain in deficit, and legacy was expected to increase further to exceed £300 million by the end of the decade, despite aggressive cost-cutting measures.
Consequently all four DGHs had been formally designated by NHS London as financially challenged trusts.
Analysis of the financial and operational performance of the six acute trusts in south-east London
- the two trusts with whole-hospital private finance initiative (PFI) schemes, Queen Elizabeth, Woolwich and Bromley Hospitals NHS Trust, had large income/expenditure and cash flow deficits and the highest legacy debt
- average productivity of the four DGHs was significantly below the top quartile performance of hospital trusts in
- there was aggregate excess bed capacity in South East London of more than 400 acute beds – the equivalent of approximately a whole DGH’s bed capacity.
Of the six lessons the rest of the NHS can learn from South East London the fourth stands out:
“…….competition and choice in contestable services may inadvertently cause deterioration in the quality of essential services provided by financially challenged trusts, and therefore widen the quality gap between the best and worst performers. Market forces alone will rarely drive trusts into voluntary agreement to reconfigure in ways that will improve quality and reduce costs. In most cases, the most likely outcome is that financially challenged trusts will suffer a downward spiral of continuing financial deficits, deterioration in the quality of care and a further widening of the quality gap. The NHS will have no alternative but to continue to fund these deficits or allow the trusts to fail.”
Few, if any of them, will ever become foundation trusts. This conclusion is important in view of the considerable emphasis placed by the coalition government on ‘making the market work’.
The coalition government’s decision to transfer commissioning responsibility from PCTs to smaller GP consortia will further weaken commissioning levers to effect service improvement across trust boundaries in emergency and network services. GP consortia will have even less expertise and commissioning experience than PCTs; information asymmetries will be even more pronounced; and understanding of how to shape the ‘quasi-market’ will be even less developed. Since GP consortia will be much smaller than PCT joint commissioning groups, and SHAs are to be scrapped, it is unlikely that GP consortia will be successful in driving major service improvement in emergency and network services.”
Sunday, May 8, 2011
David Cameron: Listen to one of your own advisers!
Prof Chris Ham
Parliament debate:
Chris Ham"May I add something briefly? The big question is not whether GP commissioners need expert advice or patient input or other sources of information. The big problem that we have had over the past 20 years, in successive attempts to apply market principles in the NHS, has been the fundamental weakness of commissioning, whether done by managers or GPs, and whether it has been fundholding or total purchasing." “………The barriers include government policies that risk further fragmenting care rather than supporting closer integration. Particularly important in this respect are NHS Foundation Trusts based on acute hospitals only, the system of payment by results that rewards additional hospital activity, and practice based commissioning that, in the wrong hands, could accentuate instead of reduce divisions between primary and secondary care.”
Kaiser Permente Model:
Integration The most distinctive feature of the KP model is the way in which it integrates care:
Integrated inpatient and outpatient care enables patients to move easily between hospitals and the community, or into skilled nursing facilities should this be needed.
Medical specialists are not tied to a particular building – such as a hospital – but provide care in the most appropriate setting. Specialists work alongside generalists in multi-speciality medical groups that help communication between physicians. There is no incentive to build up facilities and resources at the expense of other settings.
Integrated prevention, diagnosis, treatment and care. A high priority is attached to keeping people healthy and avoiding the use of hospital services. Chronic disease management programmes, where care is delivered within the framework mentioned above, help ensure that care is provided as close to home as possible. Doctors have fast access to diagnostic services in the outpatient setting and practice from relatively large medical centres where diagnostic and other equipment is easily accessible.
Friday, May 6, 2011
Cashew: Hard Nut!

Young Cashew ©Am Ang Zhang 2011

Mature Cashew ©Am Ang Zhang 2011
You probably have never seen cashew nuts sold in their shells in shops or supermarkets. Well, there is a very simple reason: the shell is extremely hard to crack. On top of that the shell when you do manage to crack open produces a black oil that is highly irritating.
I have seen simple mechanical ‘nut crackers’ in some tropical islands where young girls with good hand-eye co-ordination are employed to crack them without crushing the soft cashew inside.
Spare a thought for these girls as some of them suffered injuries as the machines are basic in design but powerful as they need to crack the very hard nuts.
Cashews like many other nuts are now known to lower LDL and prevent Gallstone formation.
Other Uses:
Many parts of the cashew plant are used. The cashew "apple," the enlarged fully ripe, fruit may be eaten raw, or preserved as jam or sweetmeat. The juice is made into a beverage (Brazil Madeira
Others:
Others:
Thursday, May 5, 2011
NHS & The Mayo Model: What if!
“The best interest of the patient is the only interest to be considered.” These words
not only resonate with anyone who has ever worked, trained or been educated at Mayo Clinic but also with medical professionals around the world who emulate Mayo’s Model of Care.
The Cockroach Catcher surprised even himself that he was still naive about the future of the NHS that he joined over 40 years ago.
Elsewhere, I stated:
Private Health Care providers all knew the value of specialist. These specialists have been known as hospital consultants in England (and the rest of the U.K.
The only reason why they now want to move into GP service is to have control over secondary care. Many Insurers have full control over the consultants and the hospitals they are allowed to operate.
Why are hospitals and the consultants not kicking up a fuss?
Here is a view:
“In the case of the consultants, a show was made of trying to make them accept much closer supervision by hospital managers, and cut back on their private work. But it soon came to seem that the real aim of doing this was to make them feel more disenchanted with working as salaried NHS employees and readier to go into business – to form doctors chambers, on the model of barristers, or other kinds of business, and sell their services to any employer, public or private, that offered them the best terms. A significant number began to plan to do so and some have begun to. And as the cuts begin to bite there will be unemployment among hospital doctors. As you will have read, consultants are among those scheduled to be laid off by St George’s
It is of course likely that after plotters plotted for nearly 20 years to have the money making part of the NHS privatized, they are unlikely to give up quietly.
Democracy is a peculiar business and there is truth that some of us know who the enemies of the people really were.
Some politician may regret too late for not taking the opportunity and grasp the three hairs on the god of opportunity. The Cockroach Catcher did spell it out not many weeks ago.
That many of the plotters in the Labour camp are now unashamedly working for private health care insurer or provider in one form or another that they did not get the votes from the PEOPLE.
There is a view that the truth of what David Cameron planned to do to the NHS was hidden from the electorate.
If that is so it would not make any difference if Andrew Lansley is replaced.
But: What if!
What if his personal experience meant that he will now do a Coca Cola and be the one PM that saved the NHS using the Mayo Model!

Dr. Charles H. Mayo and Dr. William J. Mayo
“…….Mayo offers proof that when a like-minded group of doctors practice medicine to the very best of their ability—without worrying about the revenues they are bringing in for the hospital, the fees they are accumulating for themselves, or even whether the patient can pay—patients satisfaction is higher, physicians are happier, and the medical bills are lower.”
As Doctor William Mayo explained in 1905: “The best interest of the patient is the only interest to be considered, and in order that the sick may have the benefit of advancing knowledge, union of forces is necessary…it has become necessary to develop medicine as a cooperative science.”
Related:
Tuesday, May 3, 2011
To talk or not to talk: Trauma & Human Resilience
It seems to be against common sense to suggest that talking may not be good for severe traumatic experiences. This is more so for someone brought up on psychoanalysis; yet, the evidence is clearly against talking especially in severe trauma.
In The Cockroach Catcher:
In The Cockroach Catcher:
The speaker was a Senior Registrar from the Maudsley.
"......He was a Registrar at the time of the King’s Cross fire. He was just coming out of the station when the accident happened, and so was at the front line so to speak not just as a pedestrian but also as a psychiatrist. He became interested in PTSD (Post Traumatic Stress Disorder) and did a fair bit of research on King’s Cross and other disasters.
He quoted a number of cases, including the Herald of Free Enterprise disaster. There were those who despite help of all kinds would commit suicide. Many were heroes in that they saved many lives. Yet the feeling that they did not deserve to live eventually overtook them and they committed suicide.
What was most surprising was how the group that had counselling generally faired worse, much worse than those without any counselling. The group that did best were the ones that drank, and drank a fair amount.
It was not his intention to promote vodka but he thought we could not be kept from the truth……
His research showed that talking about the incident seemed to make things worse, much worse than anyone ever imagined……”
Then he remembered Kim Phuc:
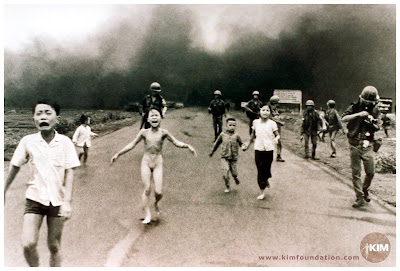 “By rights possibly one of the most damaged psychologically and physically. She underwent no fewer than seventeen operations. The photo of her running down the street of Saigon naked probably changed the course of the Vietnam War and the world’s perception of good and bad. Then came her dramatic escape in 1992 to Newfoundland and her eventual settling down in Canada. Human resilience is not to be underestimated and the imposition of psychological intervention could represent a great under-estimation of our genetical endowment. At one of her public lectures, one of the war veterans who was a helicopter gunner broke down.”
“By rights possibly one of the most damaged psychologically and physically. She underwent no fewer than seventeen operations. The photo of her running down the street of Saigon naked probably changed the course of the Vietnam War and the world’s perception of good and bad. Then came her dramatic escape in 1992 to Newfoundland and her eventual settling down in Canada. Human resilience is not to be underestimated and the imposition of psychological intervention could represent a great under-estimation of our genetical endowment. At one of her public lectures, one of the war veterans who was a helicopter gunner broke down.”Kim Phuc never had any therapy.
We have to be aware that a whole industry has sprung up based on very inexact theories and it is nice to know that the earlier findings in England have now been confirmed across the pond. In cases where mental conditions are entangled with compensation claims it becomes especially difficult to be truly objective.
On the matter of psychotherapy, a good deal of current blog comments are hostile to therapists and their methods. A good therapist is hard to come by, and should be like a wise aunt or uncle to whom one turns to for advice that one may or may not accept or act on. A good therapist needs to be intelligent and broad-minded, and mature with rich life experience. A bad therapist, on the other hand, takes over and does not allow for any leeway on how one should continue with life.
We may forget too that good therapy is for life, and may be more useful for the mentally healthy than for the mentally sick. What government or insurer would allow for that?
Here I will have to quote my Guru again:
We have to be aware that a whole industry has sprung up based on very inexact theories and it is nice to know that the earlier findings in England have now been confirmed across the pond. In cases where mental conditions are entangled with compensation claims it becomes especially difficult to be truly objective.
On the matter of psychotherapy, a good deal of current blog comments are hostile to therapists and their methods. A good therapist is hard to come by, and should be like a wise aunt or uncle to whom one turns to for advice that one may or may not accept or act on. A good therapist needs to be intelligent and broad-minded, and mature with rich life experience. A bad therapist, on the other hand, takes over and does not allow for any leeway on how one should continue with life.
We may forget too that good therapy is for life, and may be more useful for the mentally healthy than for the mentally sick. What government or insurer would allow for that?
Here I will have to quote my Guru again:
“A Therapist is like a toilet really: some may need it three or five times a week; others once in a while. Some patients may have a sort of mental diarrhoea and require therapy sessions more often.”
My only gripe is that where money is involved, one needs to be cautious: the best advice in life is free, like those from your wise aunt or uncle, if you are lucky enough to have one.
David Cameron & Mental Illness: Monitor & Bupa
I am back after traversing the Panama Canal.

Panama Canal © Am Ang Zhang 2011
Dr Grumble went VIRAL in A reader writes
“If we all take the view that Lansley's bill is unstoppable then it will be. The arguments for privatisation of healthcare just do not stack up. The emperor has no clothes. If enough people were to point that out this bill would drop dead in its tracks.”
So what about David Cameron and Mental Illness?
No, I am not suggesting anything at all although you might think so if you roll back and listen to what he said in 2009.
"…….There will be no more of those pointless reorganisations that aim for change but instead bring chaos……."
No, it is about Bupa:
The Guardian: Bupa cuts off mental illness payments after two years
Now will Monitor be doing anything about that? I doubt.
But hang on, the NHS is really safe in David Cameron’s hands as there needs to be hospitals taking back patients that Bupa does not treat.
Told you: The NHS is not going to be privatised! Not all of it any way.
My guess is that NHS 111 will be. Oooops: there may be new jobs for people to call NHS 111 as £25 a go can soon mount up and it is impossible to monitor.
Oooops, did I say monitor? Yes, Monitor may be re-launched as a QinetiQ styled company as there is so much money to be made from fining NHS Foundation Trusts. Dr David Bennett is not a medical doctor.
But, David Cameron, thanks for your faith in the NHS. And do not worry, after two years, we will be there.
Others: